By Paul Gullon-Scott BSc, MA, MSc, MSc, FMBPsS, Forensic Mental Health & Well-being Lead, Spectrum Specialist Consultancy Ltd
Forensic Focus, in collaboration with Northumbria University, is urgently seeking current and former investigators for an international well-being study to highlight this crisis. Please help protect investigators and TAKE THE SURVEY NOW.
A recent Sky News report describes an 18-year-old, Frazer McKenna, who says his life was “completely changed” after being shown a violent suicide video on a smartphone at school when he was 12. The footage lasted only seconds, but the psychological consequences have lasted years: he later received a diagnosis of complex post-traumatic stress disorder (PTSD) directly linked to the video he saw, alongside severe depression, crises, and an episode in which his family had to intervene to prevent him harming himself.
This single account is devastating in its own right. It is also a stark lens through which to examine a less visible reality: digital forensic investigators (DFIs) and related roles who routinely deal with traumatic imagery and recordings as a core part of their working day, often with inconsistent, inadequate, or culturally constrained support.
This article compares and contrasts Frazer’s experience with the occupational exposure faced by DFIs and asks an uncomfortable question: if a few seconds can profoundly injure a child, what does sustained exposure do to the professionals required to view, categorise, and evidence traumatic content repeatedly, and why are so many still expected to simply cope?
A “Few Seconds” Can Change a Life
Frazer was in Year 8 when a classmate pushed a phone into his face during breaktime; he did not choose to view the content and had no preparation for it. Sky News reports he described feeling lost and hopeless afterwards and said he did not want to speak up because peers would tell him to “man up”. His mental health deteriorated over subsequent years, including severe depression and moments of crisis, and he reported attempting to take his own life.
The report also describes enduring trauma cues: specific sounds associated with the video and everyday auditory triggers that could trigger intense anxiety and behavioural dysregulation. He describes becoming anxious, “melting down”, and lashing out. Clinically, these features align with recognised post-traumatic responses: intrusive re-experiencing, heightened arousal, avoidance, and changes in mood and cognition.
Importantly, the article frames this as not an isolated case. A consultant child psychiatrist told Sky News that similar presentations are “very, very common”, and warned that services are not equipped for the level of mental health need if children continue to be exposed to such content.
Frazer and his family are now supporting a campaign to ban smartphones in schools, arguing that a “few seconds” can change a life. That statement is difficult to contest because his story demonstrates precisely that.
Exposure Is Not an Accident, It’s the Job
Frazer’s exposure was sudden, unwanted, and developmentally premature. In contrast, DFIs are tasked with exposure often as an explicit and unavoidable component of digital investigation, and just like in Frazer’s case, this material can manifest in cases where it is not expected to be recovered.
Research and practitioner-focused literature describe digital forensics work as involving repetitive exposure to “challenging material”, including extreme violence, child exploitation, suicide, and death-related imagery or audio. In some environments, exposure is not occasional. Ethnographic research in England has described digital forensic examination as routinely involving indecent images of children, with one paper noting that more than 80% of the work undertaken by digital forensic examiners deals with images of sexual abuse of children.
This point matters: the DFI is not encountering a single shocking clip once. They may be required to open, assess, categorise, and document large volumes of content, while simultaneously maintaining evidential standards, legal thresholds, and investigative pace. And the “screen barrier” is not protective in the way outsiders assume. The work can be psychologically corrosive precisely because it combines repetition, detail, and responsibility, often with limited autonomy over pace and caseload.
Comparing Exposure: “Seconds” Versus “Sustained Contact”
1) Dose and duration
Frazer saw seconds of content and developed a severe, enduring trauma response. That illustrates a core trauma principle: impact is not determined solely by duration; it is shaped by developmental vulnerability, perceived threat, lack of control, lack of support, and meaning-making.
DFIs, however, are exposed in a fundamentally different pattern: repeated, cumulative contact. The professional may view distressing content daily or weekly as part of casework and may be required to return to the same material repeatedly for continuity, disclosure, and court preparation. This is “trauma by accumulation”, and it can be intensified by backlogs and performance pressure.
2) Choice and consent
Frazer did not consent to what he saw; the content was forced into his awareness in a school environment where he should have been protected.
DFIs technically “consent” by job role but occupational consent is not the same as psychological immunity. In many roles, the capacity to choose not to view is extremely limited. A DFI cannot ethically “look away” if the task is to identify victims, determine offence type, or secure evidence. That duty can become its own moral weight.
3) Meaning and responsibility
Frazer’s exposure was meaningless in the sense that it served no protective, investigative, or justice purpose.
For DFIs, content is often viewed in service of safeguarding and prosecution. That meaning can be protective for some, yet it can also deepen distress, because the viewer is not just witnessing harm; they are absorbing its detail while carrying responsibility for outcomes.
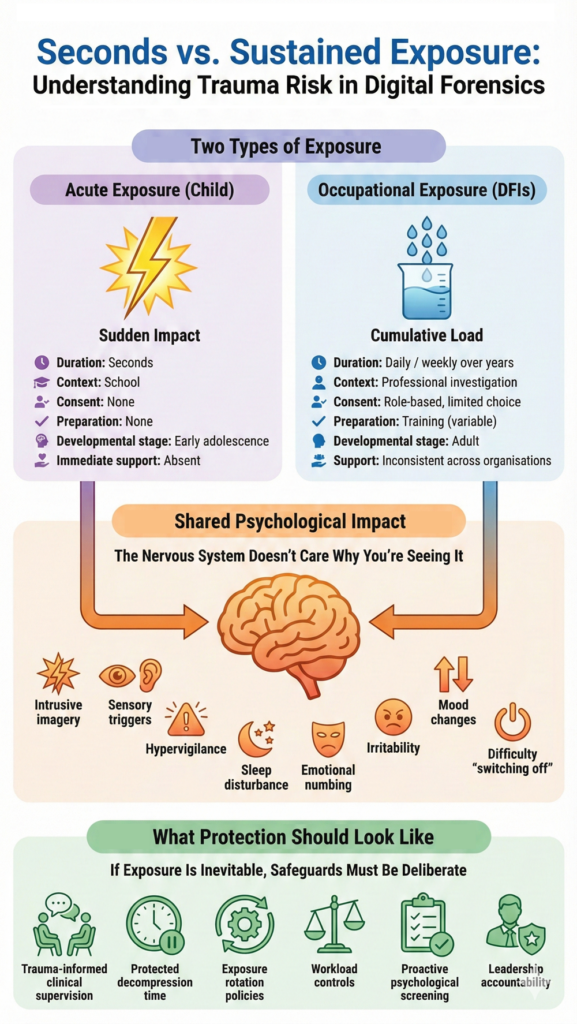
The Shared Psychological Mechanism: Triggers, Intrusions, and Collapse of Safety
Frazer’s trigger sounds linked to the video that later provoked dysregulation illustrate how traumatic memory can become sensory, involuntary, and context-free. The brain encodes certain experiences not as “past events” but as “present threats”.
DFIs frequently describe similar mechanisms, even when they are not viewing content outside work: intrusive imagery, emotional numbing, hypervigilance, sleep disturbance, irritability, and a reduced capacity to “switch off”. The work can affect intimacy, social connection, and comfort interacting with children, an especially painful irony for professionals working to protect children.
So, while the context differs radically between a child in a playground and a professional in a lab, the human nervous system is the same. That is the point: the mind does not grant immunity because the exposure is “part of the job”.
Why DFIs Don’t Get the Support They Need
The Sky News report shows a family mobilising around a child harmed by online content; clinicians validate the prevalence; policymakers debate bans and legal duties. The response, at least in public visibility, is immediate and morally clear: children should not be exposed to this.
For DFIs, the moral clarity is often inverted: because exposure is occupational, harm becomes normalised.
Several structural factors repeatedly appear in the literature and in organisational realities:
1) Hidden work and “organisational seclusion”
Previous research on digital forensic units highlights how this work can be conducted in environments that are secluded from the rest of policing and public view, with limited recognition and complex occupational identity pressures. When a role is hidden, so is the harm.
2) Stigma and the “just cope” culture
Frazer said he feared friends would tell him to “man up”. That same cultural script can persist in adult workplaces, especially those with enforcement, security, or performance-driven cultures. People learn quickly what is “acceptable” to disclose.
3) Workload pressure, backlogs, and productivity expectations
Digital forensics is not only traumatic; it is also high-throughput and deadline-driven. Workload and organisational stress are repeatedly linked to burnout risk and job strain, with consequences for absenteeism, retention, and team functioning. Even strong well-being provision can be neutralised if people have no time to use it.
4) Patchy wellness provision and inconsistent standards
Large-scale efforts (for example, ICAC-network-focused wellness work) explicitly recognise that personnel may be exposed to considerable quantities of CSAM and that agencies vary in practices designed to mitigate harm. In practice, this means access to trauma-informed supervision, clinical support, rotation policies, protected time, and proactive screening can differ dramatically between organisations even within the same country.
What Frazer’s Story Tells Us
Frazer’s case undercuts a comforting myth: that trauma is only “real” when it happens physically, face-to-face, or over a long duration. It also challenges the assumption that digital exposure is somehow less potent because it is viewed through a screen. Frazer’s trauma response emerged from mediated, second-hand content yet it still altered his development, identity, and safety in the world.
If that is true for a child exposed once, we should be intellectually and ethically consistent: occupational exposure can also injure, especially when it is frequent, cumulative, and unsupported.
A Better Standard: Support as Safeguarding for the Workforce
If organisations want sustainable digital forensics capability, well-being cannot be an optional add-on. Evidence-informed approaches emphasise targeted strategies to manage workplace stress and reduce burnout risk. In practical terms, a credible minimum standard for DFI welfare should include:
- Proactive screening and role suitability processes (not punitive, but protective), aligned with emerging agency tools and research directions.
- Structured clinical supervision with trauma-informed clinicians who understand exposure work (not just generic employee assistance)
- Protected time for decompression, peer consultation, and well-being interventions that cannot be overridden by throughput demands
- Rotation and exposure-management policies that treat high-intensity content as an occupational hazard requiring limits and recovery time
- Leadership accountability: workload, backlog, and staffing are mental health variables, not merely operational ones
- A culture shift where psychological injury is treated like any other workplace injury – anticipated, monitored, and responded to early
Final Thoughts
Frazer’s story is, in effect, a case study in what DFIs already know: digital content can be traumatising, even when exposure is brief. The difference is that DFIs are required to keep looking, often repeatedly, so that others do not have to.
If society is prepared to debate bans and legislation to protect children from harmful content, it should also be prepared to ask: what protections are we mandating for the professionals whose job is to confront that harm daily?
Anything less risks a quiet, ongoing failure of duty of care, one that costs individuals their health, families and stability – and organisations their expertise – long before anyone notices.
Paul Gullon-Scott BSc MA MSc MSc FMBPSS is a former Digital Forensic Investigator with nearly 30 years of service at Northumbria Police in the UK, specializing in child abuse cases. As a recognized expert on the mental health impacts of digital forensic work, Paul now works as a Higher Assistant Psychologist at Roseberry Park Hospital in Middlesbrough and is the developer of a pioneering well-being framework to support digital forensics investigators facing job-related stress. He recently published the research paper “UK-based Digital Forensic Investigators and the Impact of Exposure to Traumatic Material” and has chosen to collaborate with Forensic Focus in order to raise awareness of the mental health effects associated with digital forensics. Paul can be contacted in confidence via LinkedIn.